





Ten things you might not have known about The Sporting Joint
1) You can book online
2) If required, you can do your rehabilitation up to three times a week in the David Lloyd gym in Derby
3) We have a specialist Women's Health Physio to help you through all your pregnancy related issues
4) We've the yummiest humbugs in the world for patient consumption (as well as a fabulous cuppa tea or coffee!)
5) Two of our physios worked at London 2012
6) Four of our therapists have worked in full time professional sport
7) We are very easily accessible: we are five minutes walk from Derby Train Station, we have a car park outside and we're fifteen minutes walk from Derby City Centre
8) Our staff have some interesting interests! One of our physios is an archery instructor, another physio is a qualified highland dancing teacher, one of our physios has completed an artisan butchery course (not used in clinic!!) and another one of our physios competes for Great Britain at Olympic Weightlifting!!
9) We are sponsors of Derby Rugby Club, and volunteer at various sports events throughout the year for charity, making sure we give back to our local community.
10) Our logo man is called Stavros, named after Steve his creator
As an added bonus you get all this at the lowest cost of any multidisciplinary clinic in the area
HAPPY MONDAY!

Why you need to do specific exercises for rehab
Pelvic Pain in Pregnancy

Are you suffering from Pelvic Girdle Pain?……10 tips that will really help .
PGP can really take the fun out of pregnancy. However if you follow a few simple rules you can really take control again.
1. Do not stand on one leg. Now you’re probably thinking, well I don’t stand on one leg, but trust me you do, and much more than you think! For example, every time you put your knickers/socks/trousers/boots on etc you need to be sitting down. Moving something left on the floor by sliding it with one foot also constitutes standing on one leg……… Resist ladies!
2. Both legs need to go in the same direction at the same time (obviously walking is the exception to this!). So when you get out of the car, first slide the seat back as far as it will go and swing both legs out at the same time (sit on a plastic bag so you swivel easily). Turning over in bed is the same, keep both knees together so both legs roll over at the same time.
3. Avoid wearing heels. They tip all your extra weight forwards onto the front of your pelvis and that leads to a grumpy pelvis every time. Sorry, it’s just the way it is.
4. Take shorter steps and walk slower. Most of us love to walk at a fair ole pace but it’s unkind to a pelvis that is adapting to having an increased load. Learn the skill of walking slower to keep a painfree pelvis.
5. Limit stairs. As you can’t go upstairs without standing on one leg, stairs are the enemy to a woman with PGP. Plan, delegate, and limit as much as possible. Your pelvis will thank you at the end of the day.
6. Decrease the load you carry. The more weight your pelvis has to carry the more likely you are to get pain. As no one can help you carry the baby around, delegate some of the other stuff you lug from A to B.
7. Give up work earlier than you think. I know this is a controversial one but often that last month is more tiring than you can imagine and a long commute can often aggravate PGP. Maybe you can negotiate working from home one a day a week?
8. Bump lifts. This is when you lift the weight of the baby out of your pelvis by using your abdominals. It’s such a useful skill to employ when getting out of a chair, rolling over in bed or when you are just standing to relieve pain in your pelvis.
9. Pace yourself, regular rests to take the weight off your feet/pelvis are better than having a whole morning on your feet and then crashing in the afternoon.
10. Exercise. Keeping strong is always a good idea. The pelvis tends to love symmetrical exercises, including things like squats, making the sure the legs don’t go too wide. Breaststroke tends to aggravate PGP, so use a float between your legs and just do the arms so you can keep exercising.
Sally Murray, Resident Women's Health Physio @ The Derbyshire Sporting Joint
Three exercises that every pregnant woman should be doing

So, pregnancy is all rather incredible, the way the body changes and adapts to be able to grow another person inside you is all rather amazing! However, even with the easiest pregnancy the pelvic area suffers a lot of strain. These 3 exercises will help keep the front, back and underneath of your pelvis in tip top condition.
1. The underneath bit of your pelvis is known as your pelvic floor and is basically the area between your tailbone (at the back of your pelvis) and your pubic bone (at the front of your pelvis). It’s essential for soooo many things so don’t put this one off ladies, you’ll thank me I promise. Start off sitting for this one.
Squeeze round your back passage as if you’re trying to hold in wind, now squeeze as if you are trying to stop a tampon falling out, then squeeze as if stopping yourself from having a wee. Always start the contraction in that order (ie. from the back to the front). Hold the contraction for 5 seconds, relax for 5, then repeat x10. As you get stronger, build up the length of time you can hold each contraction for, aiming to hold for 10 seconds each time (and likewise if 5 seconds is too hard then hold for less).
2. The back of your pelvis gets a bit stiff and tilted as your pregnancy progresses and it will love you forever if you give it a marvellous stretch. Stand with your back against the wall and knees slightly bent. Now put a finger on your sticky out hip bones at the front of your pelvis (well they used to stick out anyway!). Tuck your tailbone forwards through your legs and feel the small of your back flatten against the wall. As you do this you should feel the bones under your fingers rock upwards. Then relax and let your tailbone stick out behind you and the hip bones will move forwards and down. Keep repeating this rocking motion 10 times or until you feel your back loosening off. https://www.youtube.com/watch?v=Oohevymcf7Q
3. Now, clearly once you move into your second and especially third trimester your abdominals have rather a challenging time! Doing a few ‘bump lifts’ every day can really help your abdominals cope and also take the strain off your back. Simply put your hands underneath your bump and lift it up towards your nose. Now engage your abdominals to keep your bump up whilst you take your hands away. Hold for the count of 3 then slowly lower the bump down. Once you get the feel of the bump lift you won’t need to use your hands at all and can simply lift the bump and lower solely using your abdominal muscles. Try doing 10 reps a couple of times a day.
Good luck ladies! And remember, if you find you are experiencing pelvic or back pain or struggling with stress incontinence then do book in to see your local Women’s Health Physiotherapist. The solution is often simpler than you think 😊
Sally Murray
Resident Women's Health Physio
@ The Derbyshire Sporting Joint
When to stop exercising due to injury

As physios we are often asked whether pushing through an injury is the right thing to do. The simplest answer is ‘it depends on what is wrong with you!’
If it’s a new injury:
Swelling: If your joint or muscle is swollen after a new injury, then you need to get the injured area up, compress it and ice it for 48 hours. There is lots of contention whether icing is good for you or not these days, but I still see huge benefit in pain reduction and swelling reduction sufficient to be able to move the area more. Avoid exercise other than activities of daily living
Instability: if your joint is giving way, you need to get it checked out by a physio or a doctor for further investigations. Avoid activity as much as possible till you’re checked out
Bruising: if the bruising is associated with pain, then avoid exercise other than activities of daily living until it settles
Wound: avoid swimming until the wound is closed and if a wound is over a joint, then you will be restricted by the doctor, either through a need for elevation of the area, or a restriction on movement.
Tendon: generally speaking even with acute tendinopathy you can still exercise, but try less loaded activities like swimming (unless it’s a shoulder tendinopathy), cycling, seated cross trainer, weight training avoiding the affected area, TRX avoiding putting weight through the affected area. No hopping, jumping or running!
Muscle injury: even with an acute injury the general advice is to ‘keep it moving’. Avoid sprinting, jumping, hopping and do light exercise like cycling, swimming, cross training, all below 60% effort. Avoid weight training of the affected area
If it’s an injury you’ve had for a long time
Persistent swelling: no area of the body should remain swollen, and therefore should definitely be checked out by a trained physiotherapist or good GP. Avoid exercise that makes the swelling worse
Instability: Hopefully you have been given some exercises to work on to improve your stability, but it’s important to avoid end of range activities/ extreme movements that load the unstable joint in vulnerable positions.
Tendon: older tendon injuries (when the acute pain has settled down) need to be loaded, initially with ‘isometric holds’. This basically means going to mid-range of movement of the joint and holding this position, preferably with a heavy weight, and best if using only the affected arm or leg. No repetitions, just holding the position.
As pain improves you can start to add in some ‘eccentric training’; eg the Achilles tendon shortens when you point your toes, so heel drops over the end of a step will lengthen it; the Quads muscles shorten when straightening the knee, so squatting will lengthen the Quads tendons; the hamstrings bend the knee, so straightening your leg from a bent knee position will lengthen the Hamstring tendons. i.e. you are working the muscle as it stretches out. The heavier the weight you can tolerate, slow and controlled, the better it is for loading the tendon. The key to doing this type of training though is to not do more than two consecutive days of loading for your tendon, and no more than four times a week. Remember that any hopping/ jumping/ running will load your lower limb tendons and therefore also ‘count’ towards your loading days.
Muscle: Make sure that you fully strengthen a muscle after injury in order to return to your previous activity. The injured side needs to be back to the strength of the uninjured side, and should have the same ability in terms of strength, power, stamina and range of movement.
Avoid sprinting/ maximally explosive activities until the muscle is fully rehabilitated or it could take you back to square one. Usually up to 80% max is within the safer zone.
When rehabilitating tendon and muscle injuries it is really important to make sure that you go through all the phases of return to activity:
1. Multidirectional activity
2. Plyometrics
3. Sport specific drills with no repercussions the following day (pain, excessive stiffness, swelling).
4. Contact as appropriate eg rugby tackling
In my opinion, the last thing you should do before returning to sport is putting the competition element back into training. It’s significantly harder to focus on technique when there is an opponent in front of you or a ball to control with skill!
DISCLAIMER: This is a really simple guide, and in no way meant to be a replacement for individualised assessment by a qualified health professional. We will not be held liable for any further injury that occurs as a result of advice taken from this blog. Please ALWAYS consult a health professional if you are in any doubt.
KATE STALKER, LEAD PHYSIO @ THE DERBYSHIRE SPORTING JOINT.
I thought cycling was good for me?!!
Injury prevention in cycling
So you’ve all the gear and only a vague idea; you’ve started cycling, training hard for the Cycle Derby Sportive, and you’re loving it… then some injuries start creeping in and you start to think ‘I thought this cycling malarkey was meant to be good for me!!’
Well, it is! But there are a few handy hints and tips we have for you to make sure that you last a bit longer past the Spring Sportive! With clickable exercise gifs you really have no excuse!!!
Stability:
Definiton: The ability to maintain a state of stableness, the property of a body that causes it when disturbed from a condition of equilibrium or steady motion to develop forces or moments that restore the original condition.
There are two main points that require good stability in order to put less strain on the rest of your body: your pelvis (and core muscles) and your shoulders (and shoulder-blade muscles).
Lower body stability: Because cyclists spend all their time bent forward, I often find their glutes don’t work as well as they should. The glutes attached around the pelvis all do different jobs:
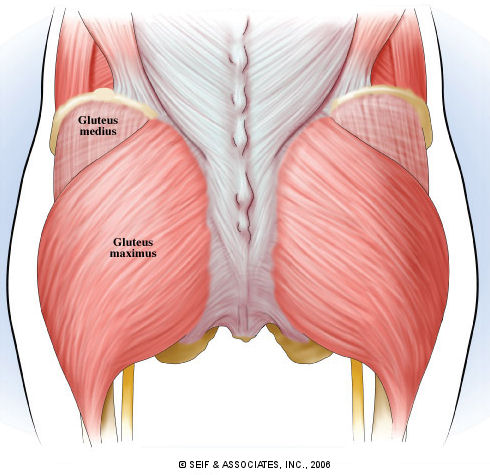
The big one at the back is the Gluteus Maximus (GMax), and it is in charge of extending your hip (moving your hip backwards).
Gluteus Medius (GMed) is a little bit further around the side of your pelvis and its main job is to help control the side to side movement of the pelvis and also control the direction in which your knees face. Your core (not your six pack muscles!) helps to keep your spine supported while still being mobile.
If GMax doesn’t work properly I often see people with lower back or hamstring issues resulting, as both areas try and pick up where GMax is lacking.
If GMed doesn’t work properly I tend to see people with back pain, groin pain, knee pain, and sometimes even ankle/ foot pain resulting.
Core stabilisers are made up of your diaphragm on top (no holding your breath!), transversus abdominis which wraps around you like a brace, multifidus which runs between each little bone of the spine and your pelvic floor, which is not only responsible for stopping you wet yourself (men and women!) but also adding to the stability of the whole system.
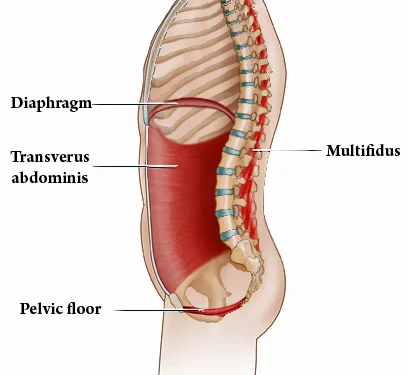
If your core doesn’t work efficiently I often see people with back or hip pain resulting
Training these areas: (Click on each exercise to watch a brief video!)
Gmax: Bridges ,single leg bridges , squats, deadlifts, single leg deadlifts, split squats, step-ups, lunges (All of these can be done with weights)
Gmed: Clams (can do with theraband), side leg lifts (can do with theraband), curtseys, sumo walks (with band)
Core: Ball work (Exercise 1, Exercise 2, Exercise 3, Exercise 4, Exercise 5, Exercise 6), planks, BOSU work (Exercise 1A&B, Exercise 2A&B)
Around the clock exercise (Great for core and pelvis).
Hamstring (can do with a straight leg too)
Upper body stability: Obviously the more stable your upper body is, the safer you are on the bike, but also the less the rest of you needs to compensate.

Your serratus anterior (SAnt) muscle helps to keep your shoulderblades under control and keep them flat against your chest wall. They are great stabilisers particularly when you’re weightbearing through your arms.
Your rotator cuff (the infraspinatus, supraspinatus, teres minor, subscapularis in the picture above!) helps control where your arm and your shoulder blade is.
The deltoid muscle is the big chunky one on the outside which is your power muscle around all the delicate structures of your shoulder. This needs to work hard when the going gets tough and the hill gets nasty and everything wants to give up!
Your trapezius (all of the parts of it) are in charge of your shoulderblade position in terms of going up/ down and in.
Your big pectoralis muscles on the front of your chest also help with the control of your arm and shoulderblade. This is a big meaty muscle and is also your champion when the going gets tough to help you control your upper body.
Training these areas:
SAnt: Push plus, weighted punches
Rotator Cuff: Cables/ Theraband exercises
Deltoids: Weights/ theraband
Traps: Wall angels (make sure your back is flat against the wall along with your forearms), pull downs (yes these work your lats too), shrugs
Pecs: Chest press (weights machine), press ups, planks, plank to press up
Good whole body exercises:
BOSU planks
BOSU mountain climber series: Exercise 1a and 1b, Exercise 2a and 2b
These are only just a suggestion for you, and by no means the Holy Grail, but I never met anyone who didn’t feel better being stronger, and it definitely will make a difference on the bike.
Best of luck with your cycling this year!
Kate
Lead Physio
The Derbyshire Sporting Joint
So…. You think you over pronate…. Relax! It’s no biggy!
Physio Tips for Runners
The Derbyshire Sporting Joint is sponsoring the medals for the Ramathon, Derby's half marathon this year on June 5th 2016. To celebrate this, I thought I would collate some of my general tips for those involved. Next month you will hear from our expert biomechanical podiatrist for her footcare tips and ideas. Kate :-)
Reflections of a physiotherapist in 2015
The end of another year is a chance to reflect, on life, work, goals for the future etc.
I started to think about all the courses and conferences I’ve been on, articles I’ve read, blogs and tweets I’ve seen, and I have to say I’m a tad confused, but also sadly worried!
As some background to me… I’m a South African physio who studied physiotherapy in my home country (graduating 2001), and then later on did a masters degree in Manual Therapy in Australia. I’ve worked 7 years full time in professional and international sport as team physio, and consulted thereafter to various sports. I now run a busy private practice in the UK but I work full time as a clinician. I would call myself a ‘hands-on-physio’ and up until recently I didn’t realise that was becoming a very much frowned upon thing to be. I also spend a lot of time with patients doing rehab exercises both in the clinic and the gym, and sometimes when I’m lucky enough to have the time, in their sporting environment.
SASMA Conference 2015
So back to the confusion: I went to one sports medicine conference in South Africa this year where the international lecturers spoke extensively about the use of manual therapy, demonstrated various techniques, explained that mechanotransduction takes place through exercise as well as handling of tissues. Taping methods were demonstrated. There was discussion about the use of dry needling/ acupuncture. There was extensive discussion about return to sport rehab exercises. There has also been a LOT of talk about fascia, at pretty much every conference I’ve been to for the last five years. Definitely the latest trend, and yes, it has been pointed out that fascia is exceptionally strong and we couldn’t hope to alter the structure of it. But manual therapists around the world are teaching fascial stretching and/ mobilisation techniques, and obviously they’re not affecting what they think they are affecting, but they must be doing something, or is this the biggest case ever of the ‘king’s clothing’? Do we just not yet understand the mechanisms of whatever people are doing to the tissue? Should we throw it out as the science hasn’t proven the method, or should we continue to practice the method to improve our skills at it, and hope that science catches up with us to explain why? I’m asking the question, and I don’t know the answer, other than how else do we learn?
Therapy Expo 2015
The next conference I went to was in the UK, a conference directed mainly at therapists. It very much reflected the trend certainly in the UK that ‘hands-off’ physio is the way people are moving. We are encouraged not to talk about pathology, as this can lead to chronic pain behaviour and delay healing. Now in certain parts of the population, this is exceptionally relevant. However, if you have a young sportsman who is virtually impossible to slow down, do we not want them to know that there is injured tissue? Do we not need them to realise the consequences of pushing on? I know that imaging does not equal pathology and visa versa but sometimes there IS pathology, and surely its best for the patient to understand it? For me there is nothing worse than another therapist in my clinic seeing a patient of mine and telling them all the things that are ‘wrong’ with them. What a nightmare when I’ve been building them up through their rehab! But equally, shouldn’t we be empowering patients to assist with their own condition when they fully understand what they are dealing with. There is also a strong push for patients not to be reliant on their ‘healing therapist’s hands’ which is music to all of our ears. But recently I saw a comment on social media when someone asked a physiotherapist if they would manip a joint which would help the painful area and the therapist responded with ‘I have better things to spend my time on’. Now this is possibly true, but are we not allowed to help make people feel better? I like to help people leave my rooms feeling like I have had an effect on the injured area, and while doing my evil ‘hands-on-treatment’ which god forbid makes them feel a little easier, we discuss what the plan is going forward, and then we work on the exercises they’re going to do, and I explain that should they not keep up their end of the bargain (their homework), whatever perceived ‘gains’ we have from the treatment will disappear as quickly as they have arrived. Personally I have tried to rehab an extremely serious injury with only exercise, and only after months and months of struggling on my own did I relent, make time, and get some help from a colleague, and the change was almost instantaneous! A little bit of hands on help in conjunction with what I was doing was the game changer.
There are obviously huge psychological issues involved with many patients, but often the ‘hands-on’ time allows us some insight into these issues, and although we are not psychologists, and I never even begin to say that we should act as such as it is far beyond our scope of pratice, sometimes the simple act of being able to tell someone what is most bothering you, often makes you feel better. If someone is in pain, is it not our duty to assist? And if beyond our scope to make appropriate onward referral?
Possibly the most disappointing thing I feel about the way in which our profession, certainly in the UK, is moving, is the disparagement of those who think differently to oneself on social media. I myself received a barrage of personal abuse (not just disagreeing with me, character attacks) from a fellow health professional on twitter who I do not know, and while I have no issue whatsoever with people disagreeing with me, the manner in which it is done should still be respectful of a colleague, and would open up to more interesting discussion. As a result I now virtually never post anything clinical on twitter for fear of another personal attack. A culture of wariness definitely exists even amongst lecturers at conferences, who anticipate the rude barrage of abuse that is often seen on social media after a lecture. And yet when it is happening to another colleague we all sit back and allow it to take place for fear of them turning on you. We can all disagree on things, and clearly I am sitting centre of one side of the the fence with regards to therapy choices, but just because we have different schools of thought does that make us wrong? My patients get better doing what I do, and yours do too. I love the fact that in my clinic I have ten different therapists who all work really differently to me, should we not be celebrating the different things we can all bring to the table rather than berating those with different philosophies? If we do not start to encourage more open discussions and support one another I am extremely concerned about the future of our profession.
Ten things I wish I had done when I was a Highland Dancer

Real Life Rehab
Getting to grips with back pain
I’ve been a qualified physiotherapist for over ten years now and I have heard literally thousands of people during that time talk about their ‘really bad back pain’. And to be honest, I never really got it. Patients would complain of severe, unremitting back pain that was there constantly. There was always a little part of my brain that thought, there is no way that this person has pain 24 hours a day.
The Actual Truth About Exercise
It was with much enthusiasm that many of my patients came in saying they had seen the BBC programme: Horizon: The Truth About exercise (http://www.bbc.co.uk/programmes/b01cywtq) in which most people who saw the programme gleaned that they only had to do 3 minutes of exercise, once a week and all would be well. In summary the guy did 3 minutes of High Intensity Training a week, and it changed his INSULIN SENSITIVITY. His aerobic capacity did not change as he is a ‘non-responder’ to exercise. That is all. What the programme did not claim was that 12 minutes of exercise a month gave you all the other benefits of exercise (and I’m talking 30 minutes of medium intensity exercise a day).
These benefits include:
Where injuries come from
My icing protocol
To rest is to rust
I’ve pretty much heard all the sayings out there with regards to injury.. ‘if it came on it’s own, it’ll leave on it’s own’, ‘rest cures all’, ‘stretching fixes everything’. But imagine your car breaks down, you park it in the garage for 3 weeks, and then 3 weeks later expect to drive it, as normal as soon as you back it out of the driveway.., a solution to the problem? Doubtful!
Chronic Pain in Sport
The Idiots Guide to Physiotherapy
Let's get moving
I see a lot of patients every day with pain, and so often their story goes... I used to go to the gym regularly, but about 3 months ago I stopped’, or ‘I just don’t have time for exercise’, or ‘I hate going to the gym because it’s boring’. My point is though, that those people are in pain for a reason: they’re weak, they’re unfit, they’re often overweight and they probably haven’t taken a deep breath in MONTHS